

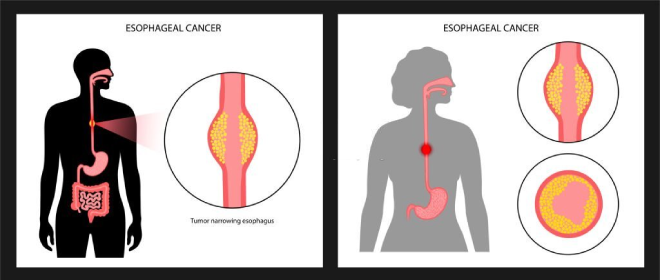
What is Esophageal Cancer?
The esophagus, a long and hollow tube connecting the throat to the stomach, plays a crucial role in the digestion process by facilitating the movement of food from the mouth to the stomach. Don’t allow esophagus cancer to define you; instead, at our Oasis Clinic discover strength and comprehensive esophagus cancer treatment in Pune.
Our experienced team is dedicated to providing exceptional care and support throughout your journey towards recovery.
Types
Esophageal cancer can occur anywhere along the esophagus. Although both genders can be affected, men are more commonly affected by esophageal cancer than women.
Don’t let Esophagus Cancer define you, Find Strength and comprehensive Esophagus Cancer Treatment in Pune at our Oasis Clinic. Take action and Reclaim your life today. Request a Consultation and let us guide you towards a path of healing.
Esophageal cancer is classified according to the type of cells that are involved. The type of esophageal cancer determines the treatment options. Types of esophageal cancer include:

Squamous cell Carcinoma: The squamous cells are flat, thin cells that line the surface of the esophagus. Squamous cell carcinoma occurs most often in the upper and middle portions of the esophagus. Squamous cell carcinoma is the most common esophageal cancer in India and worldwide.
Adenocarcinoma: Adenocarcinoma begins in the cells of mucus-secreting glands in the esophagus. Adenocarcinoma occurs most often in the lower portion of the esophagus. Adenocarcinoma is the most common form of Esophageal Cancer in the United States.
But ,There is no direct Anatomical connection between the esophagus and the gallbladder, meaning that esophageal cancer does not typically spread to the gallbladder or vice versa.
However, certain Risk factors such as Smoking, obesity, and a history of Gastrointestinal Diseases may increase the likelihood of developing both Esophageal and Gallbladder Cancers.
Symptoms
Difficulty and pain with Swallowing, particularly meat, Bread, or Raw Vegetables. At the start patient may have pain when swallowing solids. As the tumor grows, it can block the pathway to the stomach. Later on, even liquid may be painful to swallow. Advanced cases may be unable to Swallow at all.
- Pressure or burning in the chest
- Pain in the chest or throat
- Indigestion or heartburn
- Vomiting
- Frequent choking on food
- Unexplained weight loss
- Coughing or hoarseness of voice
Recognizing early Esophagus Cancer symptoms is crucial for timely intervention. Consult the Oasis Clinic, Esophagus Cancer Specialist in Pune for accurate Diagnosis and Personalized treatment plans.
Risks
Common risk factors for Esophageal Cancer are:
- Gender – Men are three times as likely to develop esophageal disorders as women.
- Age – Risk of esophageal cancer is highest after 65.
- Tobacco – Any form of tobacco use, including cigars, cigarettes, and chewing tobacco, increases the risk of Esophageal cancer.
- Alcohol – High intake of alcohol increases your risk. The risk is higher for people who smoke and drink Regularly.

- Age – Risk of esophageal cancer is highest after 65.
- Tobacco – Any form of tobacco use, including cigars, cigarettes, and chewing tobacco, increases the risk of Esophageal cancer.
- Alcohol – High intake of alcohol increases your risk. The risk is higher for people who smoke and drink Regularly.
- Diet – Eating a diet rich in fruits and vegetables lowers your risk, while eating a diet high in processed meats may increase your risk. Overeating is also associated with an increased risk.

- Obesity – Obese people are more likely to develop esophageal cancer.
- Gastroesophageal reflux disorder (GERD) – Apart from immediate effects such as discomfort, and relatively short-term effects such as oral problems, GERD is associated with a higher risk of esophageal cancer. The risk is higher the longer you have the condition and the more severe the symptoms are.
- Barrett’s Esophagus – People with chronic GERD can develop Barrett’s Esophagus, in which the squamous cells of the lower esophagus are replaced by gland cells more associated with the small intestine. This condition is associated with a significant increase in the risk of other esophageal disorders, like cancer
- Achalasia – If the sphincter between the esophagus and stomach doesn’t relax properly, it can’t stretch out all the time. Food then sits in the lower esophagus, causing irritation. Achalasia is a major risk factor for esophageal cancer.
Age, gender, Alcohol,Diet , tobacco etc can play a role in Esophagus cancer risks, but with the right care and guidance from Dr. Aditya Kulkarni, esophagus cancer surgeon in Pune, you can proactively protect yourself. Call now to schedule an appointment.
Diagnosis Tests
Once you Consult an Oncologist and tell him about your symptoms, he will guide you towards further diagnostic procedures. This might include some tests and procedures like:
Barium Swallow/ Esophagram
The patient swallows a liquid containing barium and then a series of x-rays are taken. Barium coats the surface of the esophagus, making a tumor easier to see on the x-ray.
Upper Endoscopy, also Called Esophagus-Gastric-Duodenoscopy
Upper endoscopy allows the doctor to see the lining of the esophagus. A thin, flexible tube with a light and video camera on the end, called an endoscope, is passed down the throat and into the esophagus while the patient is sedated. If there is an abnormal looking area, a biopsy will be performed to find out if it is cancerous.
Endoscopic Ultrasound
This procedure is often done at the same time as the upper endoscopy. During an endoscopic ultrasound, an endoscopic probe with an attached ultrasound that produces the sound waves is inserted into the esophagus through the mouth.

The Ultrasound is used to find out if the tumor has grown into the wall of the esophagus, how deep the tumor has grown, and whether cancer has spread to the lymph nodes or other nearby structures. An ultrasound can also be used to help get a tissue sample from the lymph nodes.
Biopsy
Other tests can suggest that cancer is present, but only a biopsy can make a definite diagnosis. A biopsy is the removal of a small amount of tissue from the suspicious area for examination.
A pathologist then analyzes the sample(s). A pathologist is a doctor who specializes in interpreting laboratory tests and evaluating cells, tissues, and organs to diagnose disease.
Computed tomography (CT or CAT) scan
A CT scan creates takes pictures of the inside of the body using x-rays taken from different angles. A computer combines these pictures into a detailed, 3-dimensional image that shows any abnormalities or tumors.

A CT scan can be used to measure the tumor’s size. Usually, a special dye called a contrast medium is given before the scan to provide better detail. This dye is generally injected into a patient’s vein.
Magnetic resonance imaging (MRI)
An MRI uses magnetic fields to produce detailed images of the body. MRI can be used to measure the tumor’s size. A contrast medium is usually injected into a patient’s vein to create a clearer picture.
Positron emission tomography (PET) scan
PET scan is a way to create pictures of organs and tissues inside the body. A small amount of a radioactive sugar substance is injected into the patient’s body. This sugar substance is taken up by cells that use the most energy. Because cancer tends to use energy actively, it absorbs more of the radioactive substance. A scanner then detects this substance to produce images of the inside of the body.
Stages
Stage 0 & I
At this stage, cancer is limited to the innermost layer i.e. mucosal lining. It has not yet reached the muscle layer. This is a very early stage and generally it is detected by chance without any symptom or signs. Additional tests are required to confirm the stage. Since it is an early stage results of cure are very good (90-95% survival).
Stage II
At this stage, cancer has reached the muscle layer. In many of these patients, surgery may be the initial treatment. Other option that is very often done is to give chemotherapy with radiation therapy to the tumor followed by surgery.
This increases the chance of cure, but, increases the risk of complications during and after surgery. However, surgery is the only treatment that can cure this cancer. The surgeon takes the decision based on the case findings.
Stage III
Stage III includes locally advanced cancers where the treatment can be surgery when it is possible. However, if some important structures like major blood vessels or heart is involved, surgery would not be possible. In these cases a combination of chemotherapy and radiotherapy is preferred.
Stage IV
Stage IV is when the cancer is spread to other organs like liver and lung. At this stage disease is treated with chemotherapy or symptomatic and supportive care, as indicated. Cancers of esophagus in the region of neck and upper part of chest are usually treated with chemotherapy along with radiation.
Treatments
Treatment for esophageal cancer is based on the type of cancer, the stage at which it is detected and overall health of the patient.
Esophageal cancer surgery
Surgery to remove the cancer can be used alone or in combination with other treatments.
Operations used to treat esophageal cancer include:
Surgery to remove very small tumors
If the cancer is very small and spread only to the inner layer of esophagus, best option is to remove the cancer and margin of healthy tissue that surrounds it. In such cases, surgery can be done using an endoscope passed down the throat and into the esophagus.
Surgery to remove a portion of the esophagus (esophagectomy)
During esophagectomy, the portion of the esophagus containing the cancer, along with a portion of the upper part of stomach, and nearby lymph nodes are removed. The remaining esophagus is reconnected to the stomach. This is known as “gastric pull up surgery”
Surgery to remove esophagus and the upper portion of stomach (esophagogastrectomy)
During esophagectomy, the portion of the esophagus containing the cancer, along with a portion of the upper part of stomach, and nearby lymph nodes are removed. The remaining esophagus is reconnected to the stomach. This is known as “gastric pull up surgery”
Surgery to remove esophagus and the upper portion of stomach (esophagogastrectomy)
During esophagogastrectomy, the surgeon will remove part of the esophagus, nearby lymph nodes and a larger part of stomach. The remainder of stomach is then pulled up and reattached to the esophagus. If necessary, part of the colon (large bowel) is used to help join the two.
There are many ways in which esophagectomy can be performed based on the location of the tumor and the expertise of the surgeon.
It involves large cuts or incisions on the patient’s body to make a big opening through which the surgery is done. It is highly painful; there is chance of increased blood loss, infection and prolonged recovery.
Dr. Aditya Kulkarni and team use a technique called VATS (Video Assisted Thoracoscopic Surgery) or Thoraco-laparoscopic Esophagectomy or Minimally Invasive Esophagectomy to give best results. In these surgeries, the entire procedure is performed using small keyhole incisions, which leads to less pain, less blood loss, faster recovery of the patient.
Using a robot, VATS surgery can be performed with improved comfort. For complete removal of tumour by open technique, the chest has to be opened with a long incision called thoracotomy. This is combined with another big incision on the abdomen called laparotomy. Thoracotomy not only causes lung related complications and severe pain immediately after surgery, but also leads to long term pain in the chest and anterior abdomen. Esophagectomy when performed by laparoscopy or robotic surgery avoids most of these complications which are mainly related to access wound.
With open surgery, visibility and access for surgical procedure is a problem, due to rigidity of the thoracic cage. There is always a limit to which ribs can be spread fracturing them and adding to long term pain. Robotic surgery is not only is done through tiny incisions, but, also give far better visibility to the surgeon. This makes surgeries far safer. Lymph nodes along recurrent laryngeal nerves are a common site of spread in patients with esophageal cancer. Surgery along these nerves can lead to nerve injury, which may lead to hoarse voice, swallowing difficulties, and postoperative lung infections. Open surgery has limitations such as two-dimensional vision, instrument rigidity, and limited surgical space. This may lead to unintended damage to the nerve. The robot with magnified three dimensional view and articulating instruments allows more controlled dissection, leading to safer surgery.
Chemotherapy is drug treatment that uses chemicals to kill cancer cells. Chemotherapy drugs may be used before (neoadjuvant) or after (adjuvant) surgery for esophageal cancer. Chemotherapy can also be combined with radiation therapy for better results.
In people with advanced cancer that has spread beyond the esophagus, chemotherapy may be used to help relieve signs and symptoms caused by the cancer. This is known as palliative chemotherapy.
Radiation therapy is most often combined with chemotherapy in people with esophageal cancer. It may be used before surgery, or occasionally after surgery. Radiation therapy is also used to relieve complications of advanced esophageal cancer, like tumour blocking the food pipe. Side effects of radiation to the esophagus include sunburn-like skin reactions, painful or difficult swallowing, and damage to nearby organs, such as the lungs and heart.
Combining chemotherapy and radiation therapy may enhance the effectiveness of each treatment. Combined chemotherapy and radiation may be used before surgery. But combining chemotherapy and radiation treatments increases the likelihood and severity of side effects.
Treatments for complications
Esophageal stent
Treatments for esophageal obstruction and difficulty swallowing (dysphagia) can include:
- Relieving esophageal obstruction. If esophageal cancer has narrowed the esophagus, a surgeon may use an endoscope and special tools to place a metal tube (stent) to hold the esophagus open. Other options include surgery, radiation therapy, chemotherapy, laser therapy and photodynamic therapy.
- Providing nutrition. Doctor may recommend a feeding tube if patient is having trouble swallowing or if having esophagus surgery. A feeding tube allows nutrition to be delivered directly to stomach or small intestine, giving the esophagus time to heal after cancer treatment.
Esophageal cancer surgery carries a risk of serious complications, such as infection, bleeding and leakage from the area where the remaining esophagus is reattached to the stomach. It is one of the most difficult among major cancer surgeries. However, the outcome of this surgery is more likely to be successful if performed by a qualified and experienced GI cancer surgeon.

Sir mere chest me halka halka dard hota tha …dard change hota tha kabhi left kabhi right side me dakaar bhi ataa tha to maine BHU me gastroenterology vibhag me dr.b.k Dixit ko dikhaya to unhone GERD Bataya aur bole tum jyada sochte ho isiliye ho tha hai unhone 1 month ka dwa Diya lekin dwa chodne ke baad firr se vahi ho rha hai my age is 25